

{kind=link}

By Gilda Salomone
Games have always been played in all cultures to amuse and distract. If you’ve ever played a quiz game like Jeopardy, you have experienced the emotional thrill of getting answers right and doing so before your opponents. Time goes by quickly, and you become completely immersed in the activity. Although all games have rules and involve competition, not all are designed solely for entertaining. When games have an educational purpose, they are called serious games. The use of games as learning tools is growing in environments such as defense, engineering, politics and health care.
Dr. Jeff Wiseman, an Internal Medicine physician at the Royal Victoria Hospital of the McGill University Health Centre (RVH-MUHC), assistant professor of Medicine at McGill University and core member of the McGill Centre for Medical Education, is currently developing a serious medical smartphone-based game called The Deteriorating Patient with the aim of helping medical students learn how to stabilize severely ill patients when on call. He gives us the nitty-gritty on serious games and their applications in medical education.
What are the benefits of using games for educational purposes?
Serious games can be a powerful tool to engage students. We are emotional people, and competition is filled with emotion. That’s why playing a game for many human beings is so exciting. It’s that thrill of just barely being able to meet a challenge and triumphing over adversity that many, not all, human beings enjoy. We become so involved in an activity that nothing else seems to matter.
Are there disadvantages to serious games?
Serious games should not be used carelessly: they can take time to develop and may lead to unintended negative learning outcomes such as learning how to win the game rather than learning how to be a better health professional. We have to choose a precise educational problem for which there is no other similarly effective teaching method. We also have to ensure this problem can be successfully transformed into a serious game. Many developers want to develop a game first and foremost without asking themselves the question ‘Why do I need this game?’
How can serious games be used to teach medical students and residents?
Serious games can be excellent training tools. They can help students prepare for emergency situations, for example. A patient’s health can deteriorate quickly, so we need to take action fast, many times with incomplete information. These stressful situations are challenging to learn and involve mental and emotional aspects. Students can practice thinking through emergencies with dolls and real equipment at the McGill Medical Simulation Centre. That’s effective, but also expensive and time consuming. Serious games, on the other hand, promise to achieve similar learning outcomes, with the benefit of being cost effective and easy to implement, particularly for less experienced learners. This would free up the Simulation Centre for use by more experienced learners.
You use a simulation called the Deteriorating Patient in a course called ERRAD (Early Recognition of and Response to Acute Deterioration), given to fourth-year medical students about to become residents. How does this simulation work?
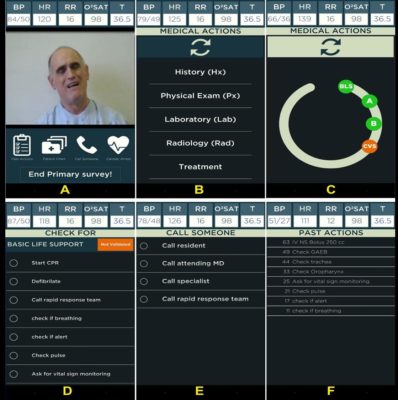
A simulation is a representation of a real-life situation: people take on roles, perform tasks and face the consequences of their decisions and actions. In the Deteriorating Patient simulation, I tell my students ‘Imagine you are the physician on first call during the night shift on an in-patient ward. You are called by the ward nurse because “Mr. Smith looks terrible, with a blood pressure of 80/60.” What do you do?’ Students have to take a series of steps to treat the patient as successfully and as quickly as possible. If you make mistakes, the patient can worsen and even die. As a tutor, I adjust the game according to learners’ level, coach them and record every action for debriefing. The idea is to offer students a safe, relevant challenge in a way that’s supportive, inspiring and mutually trusting.
Is a simulation a serious game?
A simulation becomes a serious simulation game if one adds to it the elements of competition, rules and a visible measurable goal. An example of this is “SimWars”, a competition where teams attempt to solve the same simulation scenario with the goal of saving a life fastest and with the best outcome, as judged by a panel of experts.
You are developing the Deteriorating Patient smartphone app. Why?
The main reason is, again, educational. With an app, students can practice on their own on a patient’s case over and over again until they get things right and save the patient’s life. Results are then analyzed by a tutor who gives students feedback on their recorded performances. That’s called deliberate practice with feedback. My students suggested we go further and add a scoreboard and develop an online community. I’m working in collaboration with experts in Educational Psychology, Learner’s Emotions and Computer Science and hope to be able to fully implement the app into the ERRAD course by 2017. Once the app works for medical students, we’d like to use it to teach nurses. The idea is to transform the Deteriorating Patient app into an interprofessional educational tool.
You are also a researcher at the Research Institute of the MUHC (RI-MUHC). Can the Deteriorating Patient app be used as a research tool?
We hope to get educational psychological data on adaptive expertise and learners’ emotions. Doctors have to develop two types of expertise: reproductive expertise – where you do something over and over again to a high degree of precision, and adaptive expertise – where you have to come up with quick, optimal solutions for problems that are constantly evolving. Almost all of the research in medical expertise has been in reproductive expertise. By conducting research related to adaptive expertise, we can better understand how people learn from cases that change dynamically over time and what makes them highly adaptive. We also hope to discover more about how students’ emotions can help or hinder learning.
You’ve been involved in medical education for more than 30 years. What drew you to this area?
As a physician, I can personally look after 20, 30 patients on a ward. But as an educator, I magnify the effect of my knowledge and experience by teaching many other health professionals to care for far greater numbers of patients. Medical education is one of the “basic sciences” of health professional education, just like biochemistry, anatomy and physiology. Education is a critical enabler of the translation of basic research into clinical practice. Like fresh water education is essential, but easily taken for granted. In terms of return on society’s investment, education gives you a “big bang for the buck.” Derek Bok, a former president of Harvard University, once said ‘If you think education is expensive, try ignorance.’”
Gilda Salomone is a Communications Officer at The McGill University Health Centre.