

{kind=link}

By Alex Radkewycz
In a bold and very challenging move, thoracic surgeons at Toronto General Hospital, University Health Network removed severely infected lungs from a dying mom, keeping her alive without lungs for six days, so that she could recover enough to receive a life-saving lung transplant.
This is believed to be the first such procedure in the world, made possible by advanced life support technology, a dedicated and diverse surgical, respirology, intensive care and perfusion team, as well as the grit and gumption of the patient and her close-knit family.
“This was bold and very challenging, but Melissa was dying before our eyes,” says Dr. Shaf Keshavjee, Surgeon-in-Chief, Sprott Department of Surgery at University Health Network (UHN), one of three thoracic surgeons who operated together on Melissa to remove both her lungs. “We had to make a decision because Melissa was going to die that night. Melissa gave us the courage to go ahead.”
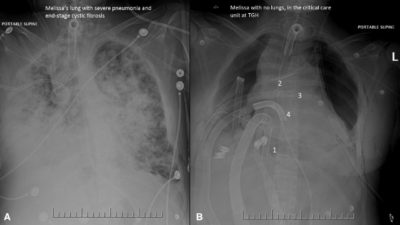
Melissa Benoit, then 32, was brought into Toronto General Hospital’s (TGH) Medical Surgical Intensive Care Unit (MSICU) in early April 2016, sedated and on a ventilator to help her laboured breathing. For the past three years, Melissa, who has cystic fibrosis, had been prescribed antibiotics to fight off increasingly frequent chest infections.
A recent bout of influenza just before her hospital admission had left Melissa gasping for air, with coughing fits so harsh that she fractured her ribs. Her inflamed lungs began to fill with blood, pus and mucous, decreasing the amount of air entering her lungs, similar to a person drowning.
As Dr. Niall Ferguson, Head of Critical Care Medicine at the University Health Network (UHN) and Mount Sinai, describes it, the influenza “tipped her over the edge into respiratory failure. She got into a spiral from which her lungs were not going to recover. Her only hope of recovery was a lung transplant.”
Melissa’s oxygen levels dipped so low, conventional ventilation was no longer enough. To help her breathe, and to gain more time until donor lungs became available, physicians placed her on Extra-Corporeal Lung Support (ECLS), a temporary life-support medical device that supports the work of the lungs and heart.
Despite this, Melissa’s condition worsened.
The bacteria in her lungs developed resistance to most antibiotics, and spread throughout her body. Her blood pressure dropped. She slid into septic shock, triggering inflammation, leaky blood vessels and reduced blood flow. One by one, her organs began to shut down. She had to have kidney dialysis.
Melissa was now on maximum doses of three medications to maintain her blood pressure, along with the most advanced respiratory support, and on last-line powerful antibiotics, the last option for patients resistant to other available antibiotics. The team was still waiting for donor lungs but, by this time, Melissa was too sick to have a lung transplant.
Dr. Marcelo Cypel, the thoracic surgeon on call that late April weekend, kept a careful watch on Melissa. On a Sunday afternoon, with the clock ticking, he kept weighing her risk of death versus the risk of trying something which had never been done before.
It was bold, but scientifically sound. Removing both her lungs – the source of bacterial infection – could save her life.
Dr. Cypel gathered his colleagues, calling in Dr. Shaf Keshavjee, Dr. Tom Waddell, Head of Thoracic Surgery at UHN, Dr. Niall Ferguson, and respirologist Dr. Mathew Binnie – all seasoned and well-known for their skills in navigating complex cases, along with Melissa’s husband, mom and dad.
The surgical team had been discussing the concept of this procedure for several years. They had observed patients with cystic fibrosis, waiting for a lung transplant, who developed severe lung infections. These infections spread through the bloodstream into their bodies, resulting in septic shock and death, despite maximum support on the ECLS device.
While the team faced many unknowns – risk of bleeding into an empty chest cavity, whether her blood pressure and oxygen levels could be supported afterwards, and if she would even survive the operation – they agreed that Melissa was a possible candidate, and that it was her only chance, although a slim one.
As Dr. Keshavjee explained, she likely still had enough strength to withstand the procedure and get better afterwards, the source of the infection was clear-cut and difficult to control in current circumstances, the family understood the risks and explained that Melissa had often told them she would want to try everything possible to live for her husband Christopher and two-year-old daughter, Olivia.
“Things were so bad for so long, we needed something to go right,” remembers, Chris, “and this new procedure was the first piece of good news in a long time. We needed this chance.”
As Melissa tells it, Chris was the one who “held my life in his hands…He had to trust in himself, knowing me, relying on past conversations, and he chose exactly what I would have told him to.”
Melissa’s mom, Sue, was so eager to save her daughter’s life, she urged the team to go ahead: “Melissa always volunteers for any study or clinical trial. She would want to do this. Let’s not waste any more time and get her into the OR.”
At 9:00 pm that Sunday evening in mid-April, a team of 13 operating room staff, including three thoracic surgeons – Drs. Cypel, Keshavjee and Waddell – removed Melissa’s lungs, one at a time, in a nine-hour procedure. Her lungs had become so engorged with mucous and pus that they were as hard as footballs, recalls Dr. Keshavjee. “Technically, it was difficult to get them out of her chest.”
But within hours of removing her lungs, Melissa improved dramatically. She did not need blood pressure medication, and most of her organs began to improve.
To keep Melissa alive, she was placed on the most sophisticated support possible for her heart and lungs. Two external life support circuits were connected to her heart via tubes placed through her chest.
A Novalung device, a small portable artificial lung, was connected by arteries and veins to her heart to function as the missing lungs. Working with the pumping heart, the device added oxygen to her blood, removed carbon dioxide, while helping to maintain continuous blood flow. At the same time, another external device, extracorporeal membrane oxygenation (ECMO), which has an external pump, circuit and oxygenator for the gas exchange of oxygen and carbon dioxide, also helped to circulate oxygen-rich blood throughout her body.
TGH is a leader in using these technologies, with the largest such program in Canada, performing up to 100 ECLS cases per year. ECLS specialists or perfusionists and MSICU nurses are specially trained in caring for patients on various ECLS devices.
Six days later, a pair of donor lungs became available and Melissa was stable enough to receive a lung transplant in late April 2016.
“The transplant procedure was not complicated because half of it was done already,” noted Dr. Cypel, “Her new lungs functioned beautifully and inflated easily. Perfect.”

For the past several months, Melissa has been steadily improving. Her previously thick hair is growing back, she can play with her daughter for whole days without getting tired, and she has not needed a walker or cane for the past month. She is still on kidney dialysis.
“It’s the simple things I missed the most,” she said, “I want to be there for Chris and Olivia, even through her temper tantrums! I want to hear Olivia’s voice, play with her and read her stories.”
The medical team is developing criteria for the select types of patients who could be candidates for this novel procedure while waiting for a lung transplantation. The report of this case by Drs. Marcelo Cypel, Shaf Keshavjee, Tom Waddell, Lianne Singer, Lorenzo del Sorbo, Eddy Fan, Mathew Binnie and Niall Ferguson on Melissa Benoit entitled, “Bilateral pneumonectomy to treat uncontrolled sepsis in a patient awaiting lung transplantation” is published online in The Journal of Thoracic Cardiovascular Surgery, November, 2016.
Alex Radkewycz is a Senior Public Affairs Advisor, Toronto General Hospital, University Health Network.