

{kind=link}
By Robyn Evan, Mariam Botros
The estimated lifetime risk of a person with diabetes mellitus developing a foot ulcer is 15–25 per cent. It is estimated that just over half of diabetic foot ulcers are infected at the time of presentation, and ulcers remain the most frequent complication of diabetes requiring hospitalization. (ref 1)A foot ulcer precedes 85 per cent of all lower-extremity amputations in patients with diabetes.
Risk factors for developing diabetic foot ulcers include peripheral neuropathy, peripheral arterial disease, foot deformity and impaired immunity related to metabolic factors. Ulcers are often caused by trauma to the extremity—usually as the result of pressure—but can also develop as a result of chemical, thermal or mechanical factors.
Well-recognized risk factors for infection in a diabetic foot ulcer are:
- Ulceration present greater than 30 days
- Previous or recurrent foot ulcers
- Renal insufficiency
- History of walking barefoot
- Positive probe-to-bone test
Infection can advance quickly and requires careful clinical follow up. Early identification and treatment of these wounds is key in preventing the cascade of human and economic burden to the healthcare system.
Preventative care
Preventing ulceration and infection should always be the goal of patients and healthcare professionals. Measures that can help prevent diabetic foot infection include:
- Patient education on proper foot care
- Glycemic control
- Blood pressure control
- Smoking cessation
- Use of prescription footwear
- Professional foot care to examine the feet at regular intervals defined by patient risk factors
For more information on prevention, visit woundscanada.ca for a downloadable brochure, available in sixteen languages.
Hidden danger
In individuals with diabetes, signs of inflammation may be concealed by several factors, meaning an infection may go unnoticed until it has progressed to a limb-threatening stage. The underlying immune disturbance and perfusion issues that are common in individuals with diabetes make it more difficult to detect inflammatory signs of infection. Diabetic sensory neuropathy might mean a patient doesn’t feel pain (and therefore will not complain about pain), while a reduced inflammatory response may decrease redness. Other signs of infection, such as presence of necrotic tissue, friable granulation tissue, increased pain, exudate and odour, can be helpful when inflammatory signs are diminished.
Diagnosing and assessing infection
Clinicians should exercise a high degree of suspicion to identify infection in its early stages, thus enabling efficient treatment and a minimized risk of limb loss. Clinicians should assess the patient, the wound and the environment to determine risk of infection; consider using Inlow’s 60-Second Diabetic Foot Screen as a tool to aid in assessment.4 Obtaining a culture is recommended if infection is suspected. The ulcer should be cleansed prior to the culture. Ideally, culture should be obtained by biopsy of tissue or bone, however this is not always practical.
A diabetic foot infection, once diagnosed, can be classified as mild, moderate or severe (see Figure 1). This requires careful evaluation of the patient (systemic symptoms), the affected limb (vascular status) and the ulcer. The severity of infection depends on the extent of the erythema, the depth of the wound and the presence of systemic symptoms (see Figure 1).
Figure 1. Classification of Infection
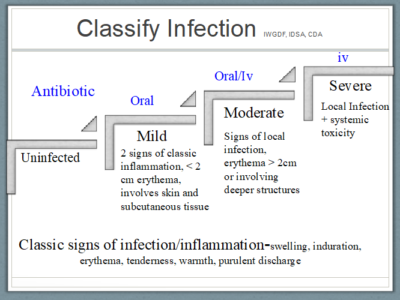
Reprinted with permission from Wounds Canada
Osteomyelitis
An infection can advance from the soft tissue by contiguous spread to the underlying bone. Osteomyelitis complicates about 20 per cent of infections. The probe-to-bone test involves using a sterile blunt probe to assess the depth of the ulcer. If gritty, hard bone is felt at the base of the ulcer in high-risk patients, there is a high likelihood of osteomyelitis.
Healthcare professionals should also consider laboratory testing and imaging to aid in assessment and diagnosis. The types of laboratory tests ordered depend on the presenting factors of the patient, co-morbid conditions and medications. X-ray imaging is a readily available test and can give information on the status of the bone or the possibility of a radio-opaque foreign body. X-ray changes related to osteomyelitis may take 2–3 weeks to develop, so serial x-ray may be required. Advanced imaging such as magnetic resonance imaging is considered the best test for diagnosing osteomyelitis.
Treating infection
Treatment of a diabetic foot infection is based on the extent and severity of the infection and co-morbid conditions (see Table 1)(figure 1). Mild infections are treated with oral antibiotics, local wound care and pressure offloading. Patients with moderate or severe infections can be considered for intravenous antibiotics and evaluated for possible surgical intervention. Antibiotics should only be used to treat the infection and not until closure of the ulcer. A guideline for antibiotic choices for the treatment of diabetic foot infection can be found in the Canadian Diabetes Association Clinical Practice Guidelines.
Table 1. Surgical vs. Medical Management
| Surgical Management if: | Medical Management if: |
| · Substantial bone necrosis
· Non-salvageable foot · No available active antibiotic · Non-correctable foot ischemia · Patient preference |
· No need for surgery
· Small and contained foot infection · Patient too unstable for surgery · Patient preference
|
Debridement of devitalized tissue is also an important part of managing these infections. This, however, is contraindicated if significant peripheral arterial disease is present.
Ideally, the management of these complex infections is best coordinated at a multidisciplinary clinic, however it is essential that front-line clinicians are able to recognize the significance of the infection and to utilize early management principles. When a multidisciplinary foot clinic is not available, appropriate referrals may include infectious disease specialists, vascular surgeons, orthopedic surgeons, endocrinologists, chiropodists or podiatrists.
Robyn Evans BSc MD CCFP is Medical Director at Women’s College Wound Healing Clinic and Medical Lead at Wounds Canada. Mariam Botros DCh DE IIWCC is CEO of Wounds Canada and a Chiropodist at Women’s College Wound Healing Clinic.